
CMS ACCESS Model: Tech-Enabled Chronic Care with Outcome-Focused Payments
The latest model signals a shift in payment for specialists

Imagine an orthopedic specialist remotely guiding a patient through rehab via a smartphone app, tracking pain and activity with wearables…and getting paid not per visit, but for actually improving that patient’s function.

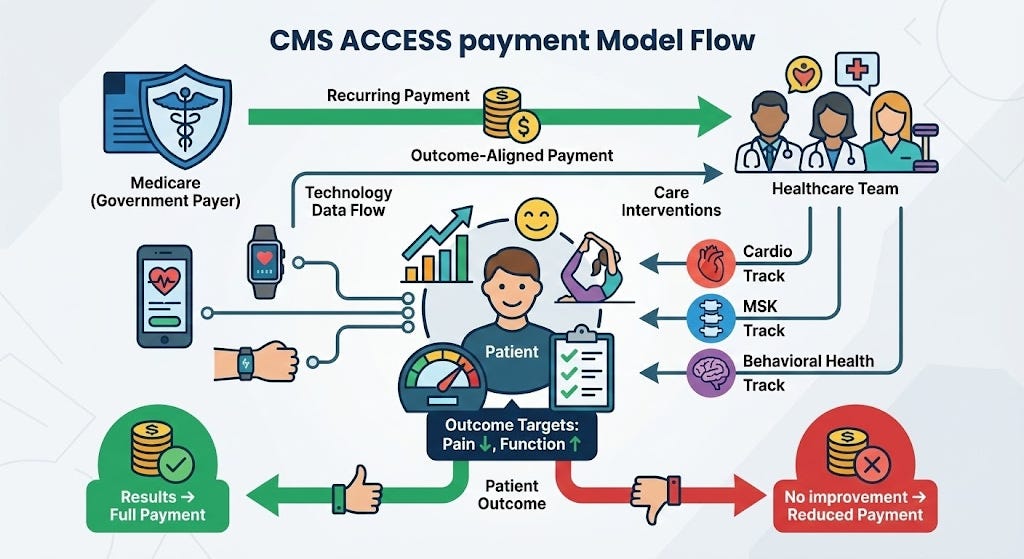
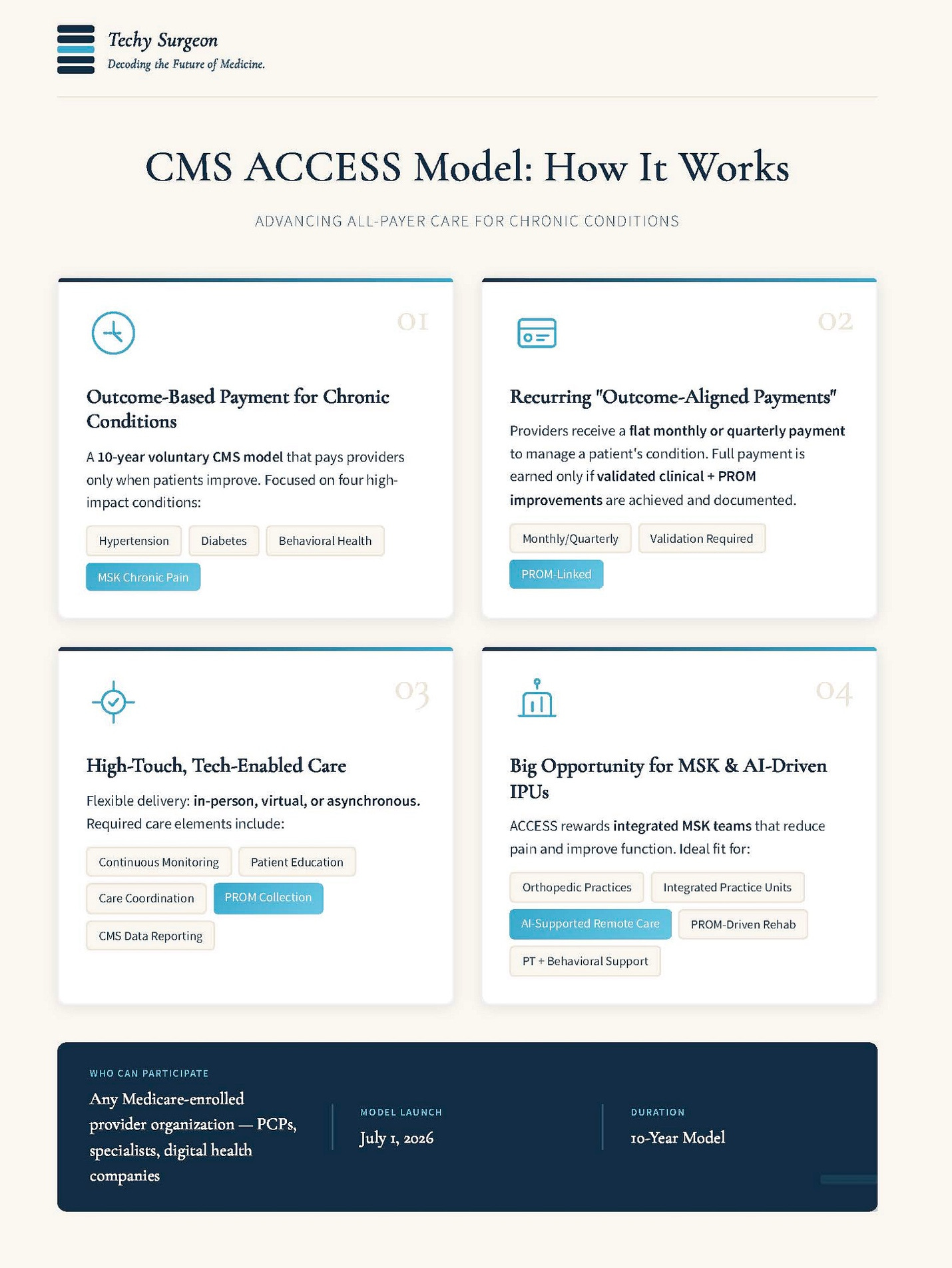
This scenario is becoming reality under Medicare’s new ACCESS Model. Launched by the CMS Innovation Center in late 2025, ACCESS (Advancing Chronic Care with Effective, Scalable Solutions) is a 10-year voluntary payment program (starting July 1, 2026) that aims to flip the script from volume to value in managing chronic conditions.1 Instead of fee-for-service billing for each appointment or procedure, participating providers receive “Outcome-Aligned Payments” – flat recurring fees to care for a patient’s condition, contingent on achieving measurable health improvements; if the patient gets better, the care team gets paid in full (and can even come out ahead); if not, Medicare will claw back or reduce the payment. This bold model rewards results over services and gives clinicians flexibility to use technology, team-based care, and proactive interventions that traditional Medicare wouldn’t reimburse – so long as those efforts lead to better patient outcomes.
What the ACCESS Model Does and Whom It Targets
ACCESS is CMS’s most aggressive test yet of value-based specialty care in the outpatient setting. It focuses on several prevalent chronic condition areas, organized into four tracks: (1) early cardio-kidney-metabolic conditions (e.g. hypertension, prediabetes, obesity), (2) cardio-kidney-metabolic conditions (e.g. diabetes, chronic kidney disease, heart disease), (3) musculoskeletal (MSK) conditions (chronic musculoskeletal pain), and (4) behavioral health (depression and anxiety). Together these affect over two-thirds of Medicare beneficiaries, so improving care here could have broad impact. Participants in ACCESS can be a wide range of provider organizations – from physician group practices and hospitals to digital health startups – as long as they enroll in Medicare, designate a physician clinical director, and comply with standard regulatory requirements (state licensure, HIPAA, FDA for any devices/software). This openness signals that CMS wants to invite non-traditional players (e.g. virtual care and health tech companies) to help manage chronic diseases, as long as they can deliver outcomes.
Patients participate voluntarily (they can sign up on their own or via referral and may disenroll anytime) and retain all their regular Medicare benefits. The ACCESS program doesn’t replace a patient’s existing doctors – it complements them. For example, a primary care physician might refer a patient with chronic back pain to an ACCESS MSK care program for specialized, tech-supported management; the PCP stays in the loop with regular electronic updates. In fact, referring providers can bill a small annual co-management fee ($30 quarterly per patient) for coordinating with the ACCESS team, encouraging collaboration rather than competition between traditional clinics and these new models. Notably, CMS allows ACCESS participants to waive patient co-pays, removing financial barriers for patients to engage in these intensive programs. And importantly, patients are free to seek any other care (seeing specialists, getting surgeries or imaging if needed) outside the program – Medicare covers those as usual. The ACCESS payment is solely for the ongoing care management and support services that historically had no easy billing code (think remote monitoring, phone follow-ups, coaching, etc.).
Outcome targets are the linchpin. Each track has defined clinical or patient-reported outcomes that must improve by a minimum amount for providers to earn full payment. In the MSK pain track, for instance, participants will need to demonstrate a meaningful improvement in patients’ pain intensity, pain interference with daily life, and functional status, as measured by validated patient-reported outcome measures (PROMs). These targets are personalized and risk-adjusted – essentially rewarding improvement from each patient’s baseline – and providers are graded on the overall proportion of their patients who meet the goals. This means an organization doesn’t have to achieve 100% success; if a high percentage of patients improve, full payments are earned (partial credit is possible if, say, 80% hit the mark and 20% don’t). CMS will publicly report the outcomes of each participating organization in a comparison directory, shining a light on which programs truly deliver better results. That transparency is designed to foster competition on quality: if one clinic’s comprehensive back pain program gets, say, 90% of patients to meaningful pain relief while another’s gets only 50%, referral sources and patients will know.
Another key design element is the payment structure and timeline. Unlike a one-time bundled payment for an episode of care, ACCESS payments are recurring (e.g. monthly or quarterly) for as long as the patient is enrolled, emphasizing continuous management. Most condition tracks envision an intensive initial 6–12 month phase of treatment, with an option to continue at a lower payment rate for maintenance thereafter<sup>1</sup>. (The exception is the MSK track – it’s expected to be an intensive one-year program with no extended phase, essentially aiming to substantially relieve the chronic pain within that period.) The model will run as a test from 2026 through 2035, with cohorts of new participants admitted in waves through the early 2030s. If it succeeds in improving outcomes and controlling costs, CMS could expand it further or make it permanent. In short, ACCESS is Medicare’s attempt to “unlock” modern chronic care: pay clinicians a steady budget to proactively keep patients healthier, rather than a la carte fees after patients get sick or debilitated.
A New Playbook for MSK Care: Integrated Teams, High-Touch Support
For musculoskeletal care providers like orthopedic surgeons, sports medicine physicians, pain specialists, and physical therapists, the ACCESS model presents an opportunity to reinvent how chronic MSK conditions are managed. Chronic back, neck, or joint pain patients today often bounce between infrequent specialist visits, short stints of physical therapy, intermittent injections, and so on, with fragmented responsibility for outcomes. ACCESS offers a chance to form an Integrated Practice Unit (IPU) or dedicated pain management team that takes accountability for the patient’s results. Under this model, a multidisciplinary team (for example, an orthopedist or physiatrist, plus physical therapists, a pain psychologist, perhaps a nutritionist and health coach) can enroll a patient with chronic knee or back pain into a comprehensive program addressing all facets of their condition. Instead of the surgeon just saying “try some PT and check back in 3 months,” the team actively follows the patient through a structured regimen of therapy exercises, behavioral strategies, medication adjustments if needed – whatever it takes to improve that person’s pain and function. Because payment is tied to the outcome, the provider team is incentivized to do more than the bare minimum – they have reason to check in frequently (even via text or telehealth), monitor progress weekly, and intervene early if the patient is plateauing. All those traditionally “non-billable” care activities (phone calls, multidisciplinary huddles, patient education on lifestyle changes) suddenly become worth doing, because they feed into success on the outcome metrics. One orthopedic group leader described it as “getting paid for all the care between the visits”, the coaching, tracking, and adjusting that really drives better results.
ACCESS encourages conservative and preventive approaches. If an integrated MSK program can spare a patient from needing surgery by achieving pain relief through less invasive means, that’s a win for the patient and for the provider’s outcome score. And if surgery does become necessary (say a patient does end up needing a knee replacement), nothing is lost – the surgery is still covered by Medicare as usual, and the patient could even re-enroll in the ACCESS program afterwards for post-operative rehab support. The model is condition-focused, not procedure-focused, so it dovetails with surgical care without centering on it. The overarching goal is to reduce disability and improve quality of life, whether or not procedures are part of the journey.
We already have evidence that this kind of integrated, high-touch model can outperform standard care. In one recent study of a digital MSK care program (a physician-led virtual IPU for chronic musculoskeletal pain), 75% of patients achieved clinically significant pain reduction and about 69% saw meaningful functional improvement after the program – even those with severe baseline pain or disability showed dramatic gains.2 For perspective, patients with very poor initial function (unable to do many daily activities) improved their functional scores by an average of nearly 600% in that program2. These are remarkable outcomes that far exceed what typical sporadic PT or routine clinic visits often yield. Another real-world analysis found that patients who participated in a comprehensive remote MSK program had almost double the odds of achieving clinically important pain relief at 1 year compared to similar patients who received usual care, with sustained improvements in function as well as lower depression and anxiety levels 5. Importantly, the intensive approach also reduced costly interventions: a 4,000-patient study noted that a digital MSK therapy program was associated with a 58% lower rate of orthopedic surgeries (and 82% fewer low-value surgeries) over 12 months versus in-person physical therapy, translating to an average savings of over $2,000 per patient per year in overall healthcare costs 3,4 These findings underscore the potential clinical and financial upside of managing MSK conditions through coordinated, outcome-driven care – exactly what ACCESS is designed to promote. Specialists who embrace this model could not only improve patient outcomes but also differentiate themselves as high-value providers, attracting referrals and payer partnerships by delivering measurably better results.

AI and Digital Health: A Force-Multiplier in Outcome-Based Care
A distinguishing aspect of the ACCESS model is how it explicitly encourages technology-enabled care. By decoupling payment from specific services, CMS is essentially saying: “Use whatever tools help your patients get healthier – apps, wearables, telehealth, remote monitoring, even AI – we’ll reward the outcomes.” This creates a fertile ground for digital health innovation in the Medicare space. Providers can deploy novel platforms and devices without worrying about billing codes for each digital touchpoint, and if those tools improve outcomes, the provider reaps the rewards (full payment, better public outcome scores, etc.). In effect, ACCESS is likely to catalyze an ecosystem of collaborations between traditional healthcare organizations and health tech companies. We may see orthopedic groups partnering with digital therapy startups, or health systems licensing remote monitoring platforms, all in service of beating the benchmark outcomes. CMS has even signaled this intent, with officials touting ACCESS as a way to foster a Medicare “health tech ecosystem” and including hashtags like #HealthTech and #AI in announcements.
Artificial Intelligence (AI) in particular is poised to be a powerful enabler in this model. While not required, AI-driven tools can help care teams manage larger populations and intervene more effectively. For instance, using machine learning analytics on patient data streams can flag when a patient is at risk of falling off track. An MSK program might analyze a combination of daily pain scores and step counts from a wearable – if the algorithm detects a concerning trend (say pain steadily rising or mobility dropping), it can alert the team to reach out before the patient’s next scheduled check-in. This kind of predictive insight allows clinicians to course-correct early, improving the likelihood the patient meets the 6-month outcome target (and thus safeguarding the payment). Some digital rehab programs already report using AI models to predict by the third or fourth week which patients aren’t likely to meet their goals, prompting extra support or treatment adjustments for those individuals. Under ACCESS, such predictive “risk stratification” could be the difference between an 85% success rate and a 60% success rate for a provider, so we can expect rapid adoption of these tools.
Beyond analytics, AI can also extend the reach of the care team through automation. Consider chatbots and virtual health coaches: a conversational AI agent could check in with patients daily (“How is your knee pain today? Did you do your exercises?”), provide basic coaching or motivational feedback, and triage issues to human providers when needed. This 24/7 low-level support ensures patients feel continuously guided – a form of “high-touch” care at scale – without overburdening clinicians with minor updates. If a patient messages at 9 pm about a pain flare, an AI assistant might respond instantly with tailored advice (e.g. a guided stretching video or a reminder of proper medication use) and flag the case for the nurse to review in the morning. By smoothing out these communications, AI can help keep patients engaged and on track between formal visits, which is crucial for chronic conditions. Digital physical therapy platforms are another example: some use computer vision algorithms through the patient’s smartphone or tablet camera to monitor exercise form and range of motion in real time, giving immediate feedback (“straighten your back” or “you’ve improved your flexibility by 10°!”). They can objectively track functional improvements (like gait speed or balance) throughout the program, providing data to the clinicians and motivation to the patient. These AI-enhanced PT tools effectively let one therapist manage many patients remotely, with the software coaching individuals on routine exercises and spotting who is struggling. Under outcome-based payment, such efficiency is gold – it can improve results and lower labor costs simultaneously.
To succeed in ACCESS, providers will likely assemble a suite of tech-enabled services: remote vital monitors, symptom-tracking apps, perhaps “AI care coordinators” running in the background to sift data and prioritize outreach. Importantly, all technology is meant to be under clinical guidance – the model stresses that digital care should be clinician-guided and accountable (no dumping patients into unproven apps without oversight). Many organizations will lean on third-party vendors for these capabilities. We’re already seeing startups offering turnkey platforms for ACCESS participants, complete with data dashboards and integrated PROM collection tools. CMS is creating an “ACCESS Tools” directory to highlight approved tech solutions and help providers find safe, effective options. The ideal approach will blend high-tech with high-touch: leverage AI and automation to extend capacity and catch issues early, while clinicians focus on empathetic, personalized care and complex decision-making. In a sense, ACCESS provides a business model for doing the right thing – spending more time and effort on patient support – by aligning financial incentives with patient health. Technology and AI will simply make it feasible and efficient to deliver this level of care at scale.
Blind Spots on Care Gaps
As with any outcomes-based payment model, the details of risk adjustment will matter enormously for equity. ACCESS aims to personalize targets based on each patient’s baseline status and clinical risk, but there is a real danger that if the risk models do not fully account for social drivers of health, functional limitations, or severe multimorbidity, programs will be implicitly rewarded for enrolling “easier” patients and avoiding the most complex ones. Vulnerable groups—such as dual-eligible beneficiaries, patients living in high-deprivation neighborhoods, or those with limited digital access—may face more barriers to completing PROMs or adhering to care plans, which could depress outcome scores even when clinicians are doing the right thing. If those factors are not adequately captured in the adjustment and payment formulas, ACCESS could inadvertently create disincentives to serve exactly the populations it hopes to help. For health systems and specialty groups, a key design question will be how to build panels, supports, and internal guardrails so that high-need patients are actively sought out and supported, rather than quietly filtered out of enrollment.
Strategic Implications: Why Healthcare Leaders Should Pay Attention
The ACCESS model heralds a new era of outcomes-focused payment that could reshape specialty care delivery. For healthcare operations leaders and hospital executives, it’s a signal that Medicare is serious about paying for value, even in areas like orthopedics and chronic disease management that have historically been volume-driven. Organizations that can reorganize care around measurable outcomes – incorporating multidisciplinary teams, deploying digital health tools, and closely tracking patient progress, stand to benefit financially and reputationally. Early adopter health systems might launch ACCESS-aligned programs (e.g. a “Medicare Comprehensive Back Pain Clinic”) to capture this opportunity, potentially gaining a market edge as regional centers of excellence for chronic care. There are certainly challenges: success under ACCESS requires investments in data infrastructure (to capture and report outcomes), patient engagement strategies for an older population, and new workflows for continuous care coordination. Providers also take on financial risk – if they don’t achieve the outcomes, they may have expended resources without full reimbursement. Careful patient selection and management will be essential, and smaller practices might partner with enabling companies or larger entities to participate without drowning in administrative burden.
That said, the policy-savvy view is that ACCESS is a proactive experiment to bend the cost curve and improve care quality at the same time. CMS will rigorously evaluate it (even incorporating a comparison group of non-enrolled patients to ensure any gains are real). If it works – i.e. shows better outcomes for patients and lower total costs – it could inform the future of Medicare payment across many conditions. If it falls short, it will yield valuable lessons. In either case, it represents a shift in mindset: paying for health results instead of services. Clinicians and leaders who have championed value-based care should find validation in this model. Those who have been hesitant may want to start developing the capabilities (PROM collection, telehealth, care management processes) that ACCESS and models like it require, because the writing is on the wall that healthcare is moving this direction.
Final Thoughts
The CMS ACCESS Model is an ambitious attempt to marry modern, tech-enabled care delivery with a value-based payment structure. For musculoskeletal and other specialists, it’s both a challenge and an invitation – a chance to innovate care pathways, break out of silos, and be accountable for what patients truly care about (less pain, better function, healthier lives). The model’s mantra is essentially: if your patients thrive, you thrive; if they don’t, you don’t. That alignment of incentives is powerful. It pushes us toward healthcare that is proactive, data-driven, and patient-centered. Hospital and practice leaders who start adapting now – building integrated teams, forging digital health partnerships, cultivating an outcome-focused culture – could lead the pack in this new landscape. And perhaps most importantly, patients stand to gain more support and better outcomes as providers strive to “earn” their wellness. As ACCESS unfolds, it will likely face growing pains and require refinements, but it represents a bold step toward a future where paying for health (instead of just healthcare) becomes the norm.
References
1. Centers for Medicare & Medicaid Services (CMS). ACCESS (Advancing Chronic Care with Effective, Scalable Solutions) Model. CMS Innovation Center. Published December 1, 2025. Accessed December 2, 2025. https://www.cms.gov/priorities/innovation/innovation-models/access
2. Grant RA, O’Connor MI, Myers P, Fiechtl J. Transforming Musculoskeletal Care: Effectiveness of a Physician-Led Telemedicine Integrated Practice Unit. Telemed Rep. 2025;6(1):300-308. doi:10.1177/26924366251382437
3. Domingues B, Pereira AP, Pradhan A, et al. Digital vs In-Person Physical Therapy in Adults With Musculoskeletal Conditions: A Retrospective Matched-Cohort Analysis of Surgery and Low-Value Surgical Rates. J Med Internet Res. 2025; (published online). doi:10.2196/82573
4. Pereira AP, Seet AM, Janela D, et al. Economic Impact of Digital Musculoskeletal Care Versus In-Person Physical Therapy: A U.S. Claims Analysis. Arch Phys Med Rehabil. 2025; (published online). doi:10.1016/j.apmr.2025.09.010
5. Wang G, Yang M, Hong M, Krauss J, Bailey JF. Clinical Outcomes One Year After a Digital Musculoskeletal Care Program: Longitudinal Study With Nonparticipant Comparison. BMC Musculoskelet Disord. 2022;23(1):237. doi:10.1186/s12891-022-05188-x
Exceptional analysis of how ACCESS flips the incentive structure for chronic care. Your point about risk adjustment equity is the cricial tension here: if CMS doesn't fully capture social determinants and functinal limitations in the outcomes formulas, providers face a perverse incentive to enroll healthier patients who are more likley to hit improvement targets. The model brilliantly solves the fee-for-service misalignment, but it could accidentally create selection bias that leaves the most vulnerable exactly where they started. The blind spot you identified around care gaps may be ACCESS's biggest design flaw if those risk models aren't robust enough to protect high-need populations.