
On JAMA's ACCESS Perspective: Bone Health Was the Missed Track
The potential and pitfalls of the new CMS Model

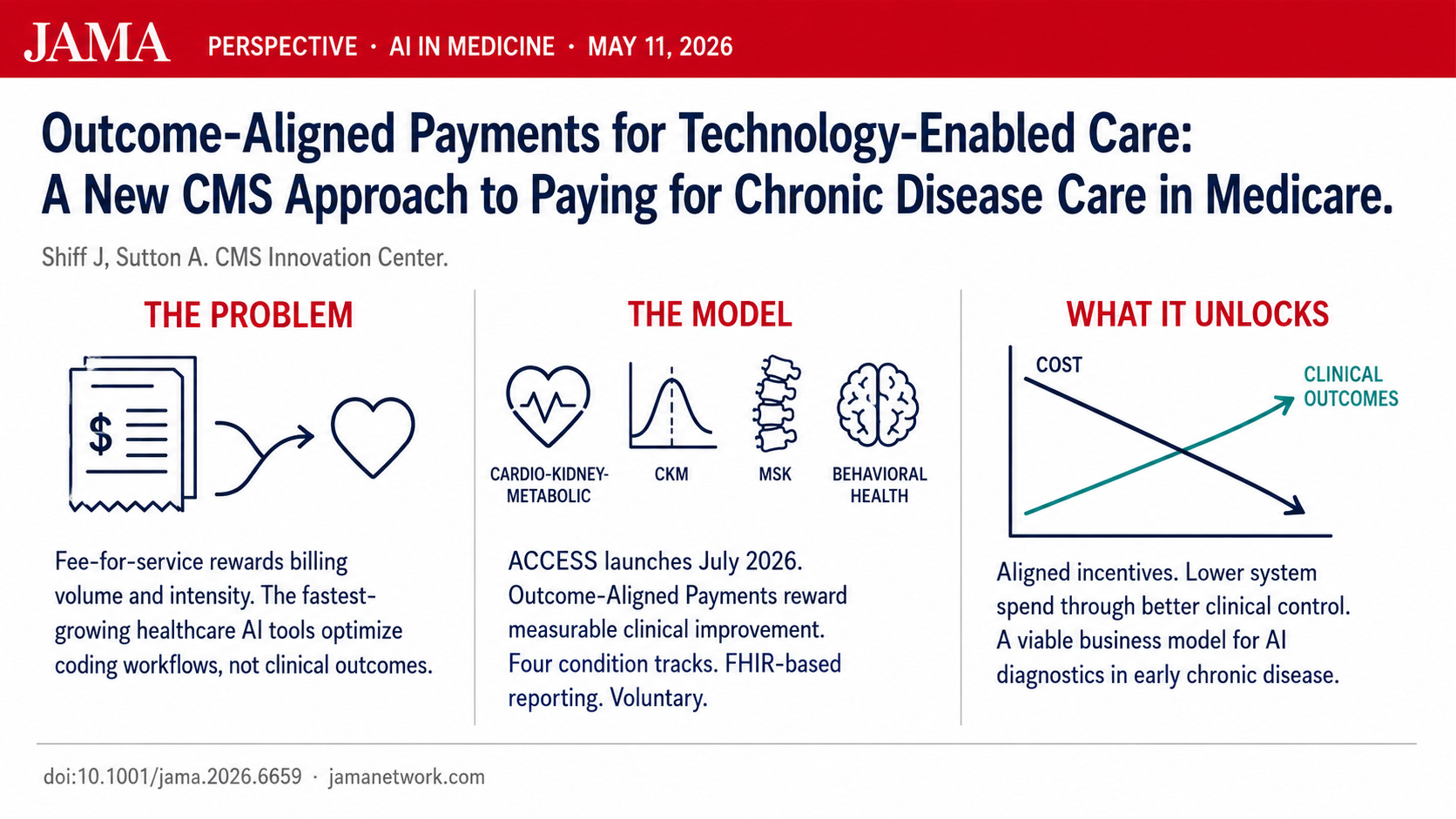
Jacob Shiff and Abe Sutton at the CMS Innovation Center published a JAMA Perspective today walking through the logic behind the ACCESS Model and Outcome-Aligned Payments [1]. It is a fairly clear articulation of how the team thought about this model and worth a read.
I personally find the core argument compelling. There is no question that fee-for-service has been distorting the technology roadmap in healthcare for years. (Does your product have a CPT code?) The fastest-growing AI products in our space optimize billing rather than clinical outcomes, because that is what the payment system rewards [2]. This has been an intractable problem, and ACCESS is a bold attempt to bend the incentive structure toward something better.
I do think there are improvements still to be made.
The track payments are low. That may be a feature, not a bug, since one of the goals is to drive efficient technology-enabled care delivery. But the MSK rates are quite low for a track that includes chronic musculoskeletal pain, which is one of the most prevalent and functionally limiting conditions in Medicare. Musculoskeletal disorders are the leading cause of disability in the United States and affect more than half of adults over age 18 and roughly three-quarters of adults over age 65 [3,4]. It is also the track that has a substantial evidence base confirming MSK virtual programs substantially reduce cost. The economics should be strong enough to support meaningful longitudinal engagement.
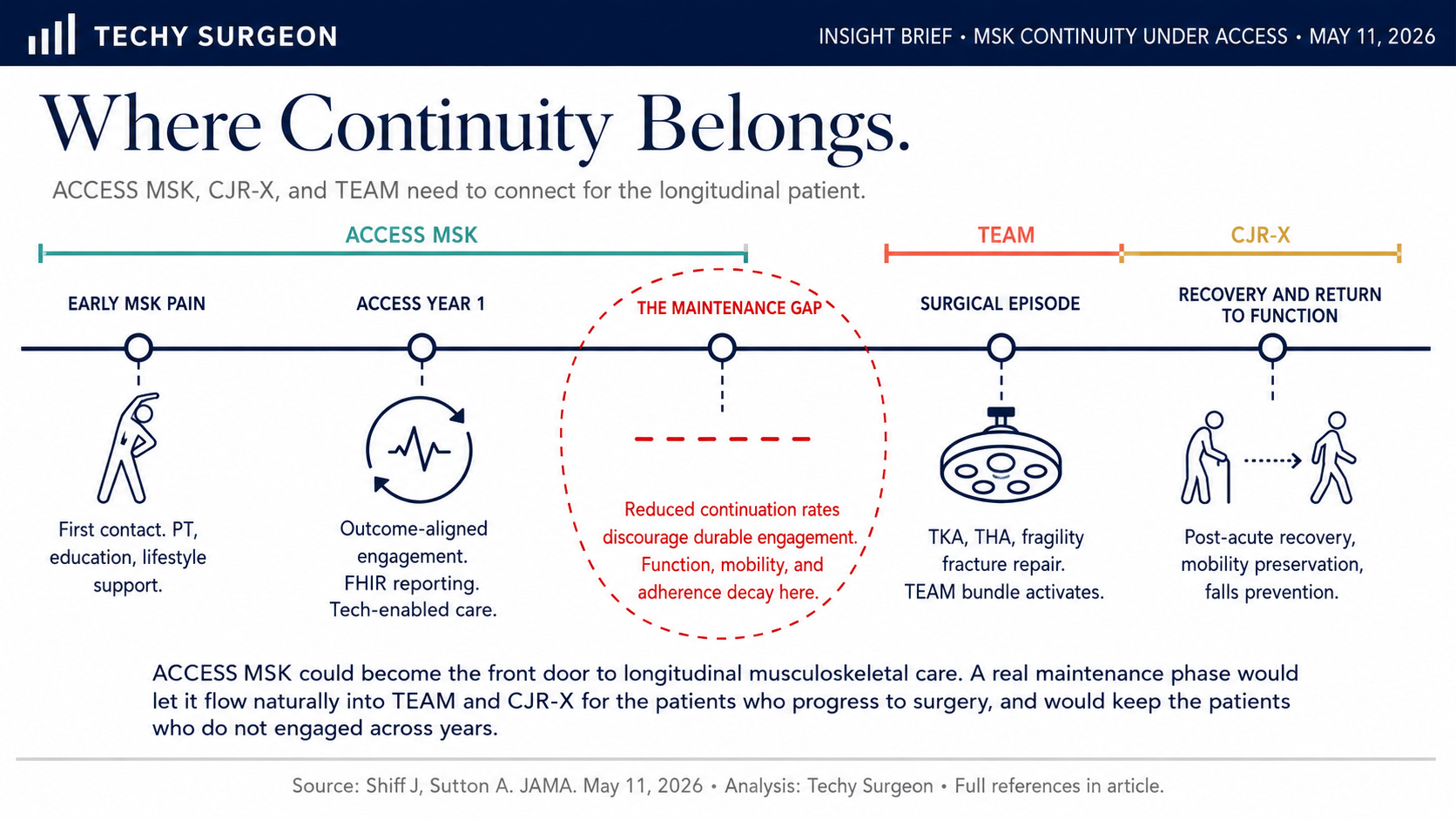
The absence of a true maintenance phase for MSK is a problem. Patients with chronic musculoskeletal disease benefit from continuity. An annual care period with reduced continuation rates makes the economics harder, and it also represents a missed opportunity for the kind of long-term engagement that actually preserves mobility and function over time. Year-over-year engagement would also have made for a compelling case for MSK to flow into the CJR-X and TEAM bundled-payment models [5,6], which I have written about previously as a connected family of models [7].
The bigger missed opportunity is bone health. I strongly believe there was a missed opportunity to include a dedicated BONE HEALTH track paired with falls prevention. We have roughly 300,000 hip fractures a year in the United States [8,9]. Less than 25% of patients who should be on osteoporosis treatment after a fragility fracture have that gap closed for them, and the rate has been trending in the wrong direction for two decades [10]. Multistakeholder consensus guidelines call for pharmacologic therapy, weight-bearing exercise, and structured falls-prevention programs after a fragility fracture, and the system consistently fails to deliver any of these reliably [11]. A dedicated ACCESS track would have been a tremendous coordination opportunity for patient-reported and care-proxy-reported falls and functional outcomes. It also would have paired naturally with existing HEDIS Osteoporosis Management in Women Who Had a Fracture (OMW) [12] and Medicare Star Ratings measures, creating an easy springboard for collaboration between ACCESS organizations, value-based organizations, and health plans on tech-enabled services.
See the JAMA article PDF below
All that said, we are very excited to participate at RevelAi Health. The MSK track of ACCESS is the first time Medicare has created a payment pathway that fits how technology-enabled musculoskeletal could be delivered at scale with the outcome at risk, and the work ahead is the work we want to be doing.
References
[1] Shiff J, Sutton A. Outcome-Aligned Payments for Technology-Enabled Care: A New CMS Approach to Paying for Chronic Disease Care in Medicare. JAMA. Published online May 11, 2026. doi:10.1001/jama.2026.6659
[2] Anderson JP, Couture SJ, Louis JF, Wiltz J, Sheingold S, Smith SR. Opportunities for Technology-Enabled Care: Economic and Payment Issues. Office of the Assistant Secretary for Planning and Evaluation; December 4, 2025. https://aspe.hhs.gov/reports/opportunities-technology-enabled-care
[3] United States Bone and Joint Initiative. The Burden of Musculoskeletal Diseases in the United States (BMUS), Fourth Edition. https://www.boneandjointburden.org/fourth-edition
[4] GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204-1222. doi:10.1016/S0140-6736(20)30925-9
[5] CMS Innovation Center. Transforming Episode Accountability Model (TEAM). https://www.cms.gov/priorities/innovation/innovation-models/team-model
[6] CMS Innovation Center. Comprehensive Care for Joint Replacement Expanded (CJR-X) Model. Proposed in FY2027 IPPS Proposed Rule, April 10, 2026. https://www.cms.gov/priorities/innovation/innovation-models/cjr-x
[7] Peán C. The CMS MSK Triad: How TEAM, CJR-X, and ACCESS Fit Together. Techy Surgeon Substack. [Insert link to prior article]
[8] Centers for Disease Control and Prevention. Older Adult Falls: Facts and Stats. https://www.cdc.gov/falls/data-research/facts-stats
[9] Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22(3):465-475. doi:10.1359/jbmr.061113
[10] Solomon DH, Johnston SS, Boytsov NN, McMorrow D, Lane JM, Krohn KD. Osteoporosis medication use after hip fracture in U.S. patients between 2002 and 2011. J Bone Miner Res. 2014;29(9):1929-1937. doi:10.1002/jbmr.2202
[11] Conley RB, Adib G, Adler RA, et al. Secondary Fracture Prevention: Consensus Clinical Recommendations from a Multistakeholder Coalition. J Bone Miner Res. 2020;35(1):36-52. doi:10.1002/jbmr.3877
[12] National Committee for Quality Assurance. HEDIS Measure: Osteoporosis Management in Women Who Had a Fracture (OMW). https://www.ncqa.org/hedis/measures/osteoporosis-management-in-women-who-had-a-fracture/