Thank you Shaleen Vira, MD, MBA, Audley Mackel III, Nick Lella, Darren Michael, and many others for tuning into my live video with Edward M. DelSole, MD! Join me for my next live video in the app.
A spine surgeon in rural Pennsylvania just found out his entire practice was selected for a mandatory CMS payment model he’d barely heard of. His Medicare Part B reimbursement—all of it, not just the episodes in question—is now subject to adjustments of up to 9% based on how his low back pain patients do over time. He didn’t opt in. There is no opt out.
This is not a hypothetical. It’s happening now to an estimated 8,600 physicians across orthopedic surgery, neurosurgery, pain management, anesthesiology, and physical medicine and rehabilitation. And it’s just one of five policy forces converging simultaneously on spine care economics.
I sat down with Dr. Edward Del Sole—spine surgeon, former Geisinger faculty, and author of the new Substack newsletter The Spinal Column—for a live conversation about what’s coming. Ed and I trained together at NYU, back when we were the guys pulling paper charts at Jamaica Hospital. The world has changed. What follows is a distillation of that conversation, supplemented with primary sources, because the policy landscape facing spine surgeons right now deserves more than casual awareness.
The Convergence No One Is Talking About
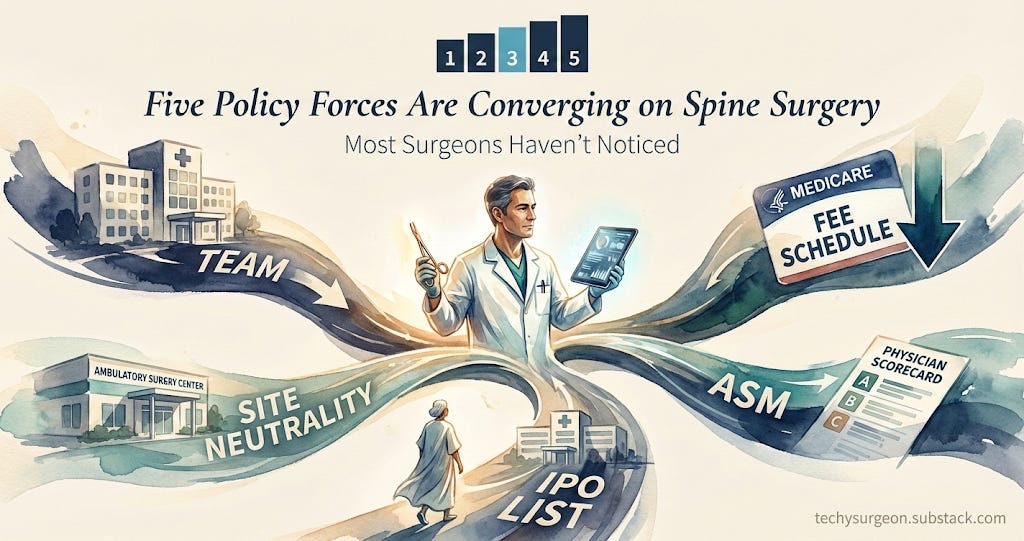
Ed’s debut article on The Spinal Column identified five policy forces reshaping spine surgery economics simultaneously. It’s worth naming them together, because their compound effect is greater than any single policy suggests:
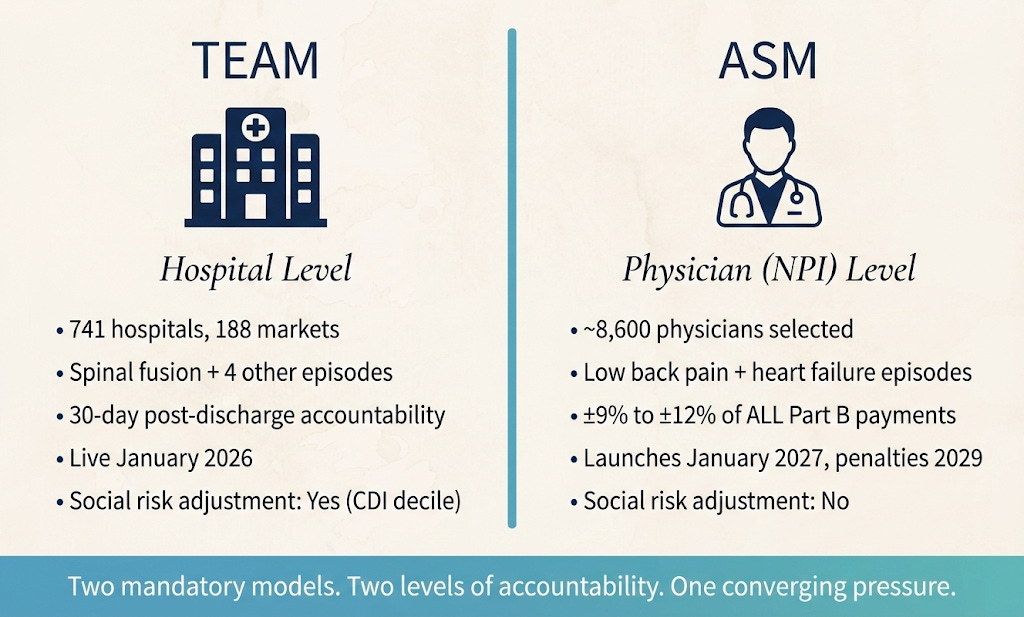
The Transforming Episode Accountability Model (TEAM)—a mandatory bundled payment program launched January 1, 2026, holding roughly 741 acute care hospitals in 188 markets accountable for surgical episodes including spinal fusion, from admission through 30 days post-discharge. Site neutrality expansion, which continues to compress the payment differential between hospital outpatient departments and freestanding offices. The inpatient-only list elimination, migrating more procedures to outpatient settings. Physician fee schedule erosion—a 33% decline in real-dollar Medicare physician payment since 2001, according to the AMA. And the Ambulatory Specialty Model (ASM)—the one that caught Ed’s practice by surprise.
Any single one of these warrants strategic attention. Together, they represent a structural transformation of how spine care is financed, measured, and delivered under Medicare.
The Ambulatory Specialty Model: Why the Employment Shield Is Dissolving
ASM is the policy that should keep spine surgeons awake at night—and that most haven’t yet internalized. Here’s why.
Unlike TEAM, which operates at the hospital level, ASM is evaluated at the individual TIN/NPI level. Every physician. Individually scored. No hiding behind institutional averages. The model launches January 1, 2027, with payment adjustments beginning in 2029, ranging from –9% to +9% of all Medicare Part B payments—scaling to –12% to +12% by 2033. CMS will retain 15% of the total risk pool as built-in program savings, meaning this isn’t budget-neutral like MIPS. The government is designed to win.
Ed put it bluntly during our conversation: “If you are a practicing clinician and you’ve been selected for ASM, you would be a fool to push it off even for a minute.”
He’s right. The requirements are concrete and operational. For low back pain episodes, clinicians must collect Oswestry Disability Index scores and demonstrate functional improvement over time. They must screen for health-related social needs. They must establish collaborative care agreements with primary care physicians. And they’re scored on episode costs—spending they may have limited ability to control once a patient leaves their office.
What struck Ed most—and what should strike every employed surgeon reading this—is what he called the dissolving “employment shield.” Historically, surgeons employed by health systems could rely on institutional infrastructure to manage quality reporting, MIPS compliance, and payment model participation. ASM breaks that pattern. It evaluates you, the individual clinician, regardless of your employment arrangement. As Ed noted: “Even as an employee, you are going to be responsible for the result here.”
The Scorecard Gap: What You Don’t Know Is Costing You
One of the most revealing moments in our conversation came when we discussed a question from Darren Michael of Forte Analytics: Do physicians actually look at their MIPS scores?
Ed’s answer was striking in its candor. At Geisinger, across five years of academic practice, MIPS was a word he “never really heard.” The institution handled it in the background. When he transitioned to private practice, he discovered he needed to personally enroll. And even now, enrolled in MIPS, he described a system that delivers no usable scorecard to his inbox, no integration with his daily workflow, no actionable intelligence about how his patients are actually doing relative to peers.
This is the gap that ASM will expose. Under ASM, clinicians will be scored relative to other specialists in their geographic region using decile-based benchmarking. If you don’t know your current performance on episode costs, patient-reported outcomes, and functional status improvement, you’re operating blind in a game where the stakes are real and the clock is already running.
The infrastructure to deliver that intelligence—to surface a clinician’s performance on the measures that actually matter and then connect it to guideline-concordant recommendations for improvement—doesn’t exist natively in most EHR platforms. It’s one of the areas where purpose-built tools could make the difference between a 9% penalty and a 9% bonus, but only if clinicians engage with the data before 2029.
The Social Determinants Paradox
Here’s an inconsistency worth scrutinizing. ASM mandates screening for health-related social needs—an acknowledgment that non-medical factors drive outcomes and costs. Yet the model includes no meaningful risk adjustment for social determinants in its cost benchmarks.
TEAM, by contrast, incorporates a community deprivation index decile into its target price risk adjustment. ASM does not. CMS is effectively telling clinicians: identify the social factors affecting your patients, but don’t expect us to account for them when we score you on cost.
Ed and I spent time on this tension. The research is clear—patients with adverse social determinants are less likely to complete patient-reported outcome measures, more likely to have ED utilization, and more likely to experience complications that drive episode costs. Penalizing clinicians who serve these populations without adjusting benchmarks accordingly is a policy choice with equity implications that deserve continued advocacy.
The practical response, in the interim, is to both screen and act. Organizations like Understood Care—which partners with practices to deploy medical advocates who help patients navigate insurance, transportation, and care access using the community health integration CPT code (G0136)—represent one model for extending the care team without adding burden to the clinician.
The Fee Schedule Erosion You Can’t Ignore
Behind all these model-specific dynamics sits a structural reality that Ed described in terms any practice manager would recognize: “You cannot really earn your money and your lifestyle by just seeing patients and even just doing surgery anymore.”
The numbers support the claim. The AMA reports that Medicare physician payment has declined 33% in inflation-adjusted terms since 2001, while practice costs have risen approximately 39% over a similar period. The 2025 physician fee schedule applied an additional 2.83% cut. The 2026 schedule avoided further cuts but did not close the gap. Medicare physician reimbursement remains the only major healthcare payment category not tied to an annual inflation index.
Meanwhile, physician compensation represents roughly 6–9% of total healthcare expenditure. The United States spent $5.3 trillion on healthcare in recent years, concentrated in hospital care and clinical services—categories where spending has continued to grow. Cutting physician pay while administrative and facility costs remain largely untouched doesn’t address the primary cost drivers. As Ed put it: “Trust in God, and all others must come with data.”
For private practices, this fee schedule erosion compounds the other four forces. Margins compress from the revenue side while compliance requirements expand from the regulatory side. The strategic calculus for many independent surgeons is increasingly stark: invest in infrastructure to win under value-based models, or accept slow financial attrition.
The Clinical AI Question: Where Technology Actually Helps
Our conversation pivoted from policy to technology—and to the question every clinician is quietly asking: where does AI actually make a difference in my practice?
Ed identified three domains. Surgical planning, where AI-driven preoperative modeling and robotic assistance are already transforming complex spine reconstruction. Patient communication, where asynchronous, AI-augmented care coordination can extend the care team without adding staff. And clinical triage—the “AI-powered front door” that routes patients to the right clinician or care pathway before wasting a visit, a copay, and a referral.
That last point deserves emphasis. Ed described a scenario any orthopedic surgeon would recognize: a patient calls their health system complaining of knee pain, gets routed to a joint reconstruction surgeon expecting a 70-year-old with arthritis, and instead encounters a 22-year-old with an ACL tear who needs a sports medicine physician. Wasted visit. Wasted copay. Delayed care. An intelligent triage system—one that understands clinical context before scheduling—could prevent this entirely. The technology exists. The integration challenge is real but not insurmountable.
The elephant in the room, as always, is the electronic health record. Epic’s recent ambient scribe rollout and pre-charting tools signal that the dominant system of record is moving into territory previously occupied by startups. The pattern is familiar: incumbents arrive late with good-enough solutions that benefit from built-in distribution. For innovators, the path forward requires solving problems the EHR won’t solve well—care coordination beyond the four walls, regulatory compliance workflows, outcomes intelligence, AI-powered patient engagement across episodes. The startups that survive will be those that don’t compete with the system of record on documentation but instead extend care delivery into the spaces where the EHR has no presence.
What Comes Next
The convergence of these five forces isn’t theoretical. TEAM is live. ASM participant lists arrive this summer. Fee schedule erosion continues. Site neutrality and IPO list changes are accelerating the shift to outpatient care. And the infrastructure to succeed under these models—the outcomes tracking, the care coordination, the intelligent patient engagement—takes time to build.
Ed’s closing thought captures the urgency: “To win the ASM game, you need to be strategizing like yesterday about how to get there, because it’s going to require not just your thoughts. It’s going to require active implementation, development of a legitimate strategy, potentially capital expense.”
The surgeons who prepare now—who understand their episode costs, establish care coordination agreements, invest in outcomes infrastructure, and begin collecting the measures that will determine their payment adjustments—will have a structural advantage over those who wait. The employment shield is dissolving. The scorecard is coming. The question is whether you’ll be ready to read it.
Christian Pean, MD, MS is CEO and Co-Founder of RevelAi Health, Executive Director of AI & IT Innovation at Duke Health, and Assistant Professor of Orthopaedic Surgery at Duke University. He writes the Techy Surgeon newsletter on clinical AI and health policy for surgeons and health system leaders.
Dr. Edward Del Sole is a spine surgeon at Keystone Spine and Pain Management in Reading, Pennsylvania and author of The Spinal Column on Substack.
Disclosure: Dr. Del Sole serves in an advisory capacity to RevelAi Health and uses its platform in his clinical practice. The policy analysis in this article reflects the authors’ independent perspectives.