
The Quantified Few
Wearables and longitudinal data are becoming a new surface for care. The question is whether that surface reaches the patients who need it — or just the worried well who can afford it.

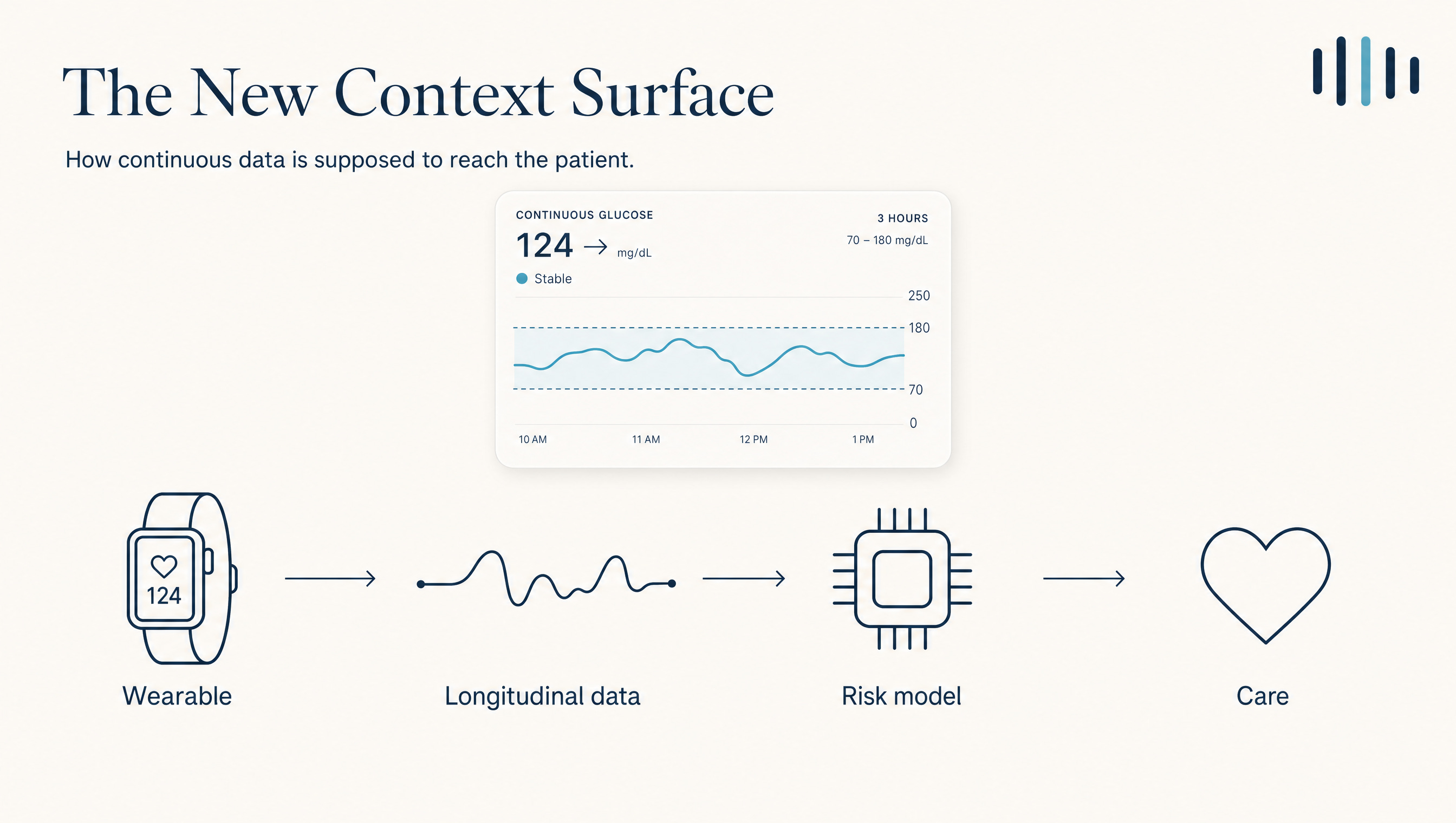
A decade ago a patient walked into clinic carrying a memory and a paper log. Today a growing minority arrive with a continuous record: heart rate, sleep, glucose, gait, oxygen. The signal that used to vanish when they left the room now persists. This is new. For the first time the context that shapes a chronic disease is legible between visits, not only during them. The surge in consumer wearables, now fused with clinical-grade continuous monitoring, has created a new clinical context surface.
The upside is real. Continuous glucose monitoring lowers HbA1c in type-2 diabetes managed in ordinary primary care; a randomized trial in JAMA found a meaningful reduction and nearly doubled time-in-range against fingersticks.1 Meta-analyses put the effect at modest but consistent,2 and a synthesis of 106,261 patients found telemonitoring cut systolic blood pressure by about 5 mmHg and HbA1c by roughly 0.4 points.3 Most chronic disease is won or lost between appointments, so a continuous read on those weeks counts as the most important new instrument in a generation.
There is a catch that should make every builder pause. The device alone does little. An updated meta-analysis of randomized trials of wearable-based remote monitoring found no significant effect across six clinical outcomes, and the interventions that worked were the ones built around behavior-change models and human coaching.4 What moves outcomes is the care built around the data. That point returns later.
i.Who is actually wearing it?
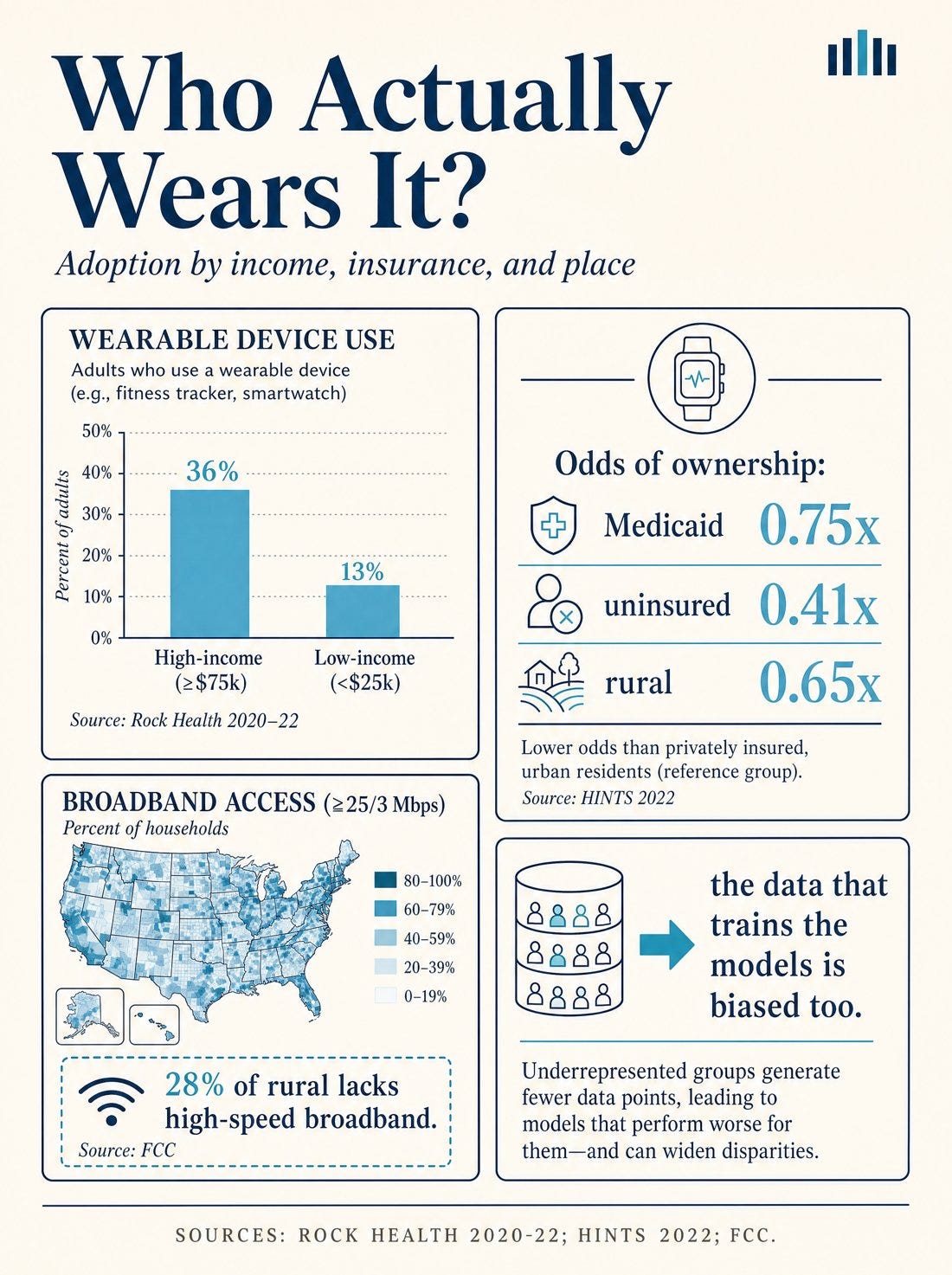
Roughly a third of U.S. adults use a wearable to track health, and that third is not a cross-section of the country. The largest consumer survey to date, nearly 24,000 people, found ownership climbing with income and education and falling with rural residence. Households earning over $200,000 had more than double the odds of ownership. Being on Medicaid lowered the odds (0.75×), being uninsured lowered them further (0.41×), and living rurally lowered them again (0.65×).5 A national analysis described wearable users as the “younger, healthier, wealthier, more educated, technoliterate,” with other groups “left behind.”6
The pattern points at the worried well. Adoption runs highest among people optimizing an already-good baseline (as I playfully quipped earlier this week). In one emergency-department survey, wearable users were younger, wealthier, and notably less likely to carry hypertension, hyperlipidemia, or diabetes than non-users.7 The patient with three uncontrolled conditions and no room in the budget for a $359 membership is the one a continuous signal could help most, and the one least likely to be holding it.
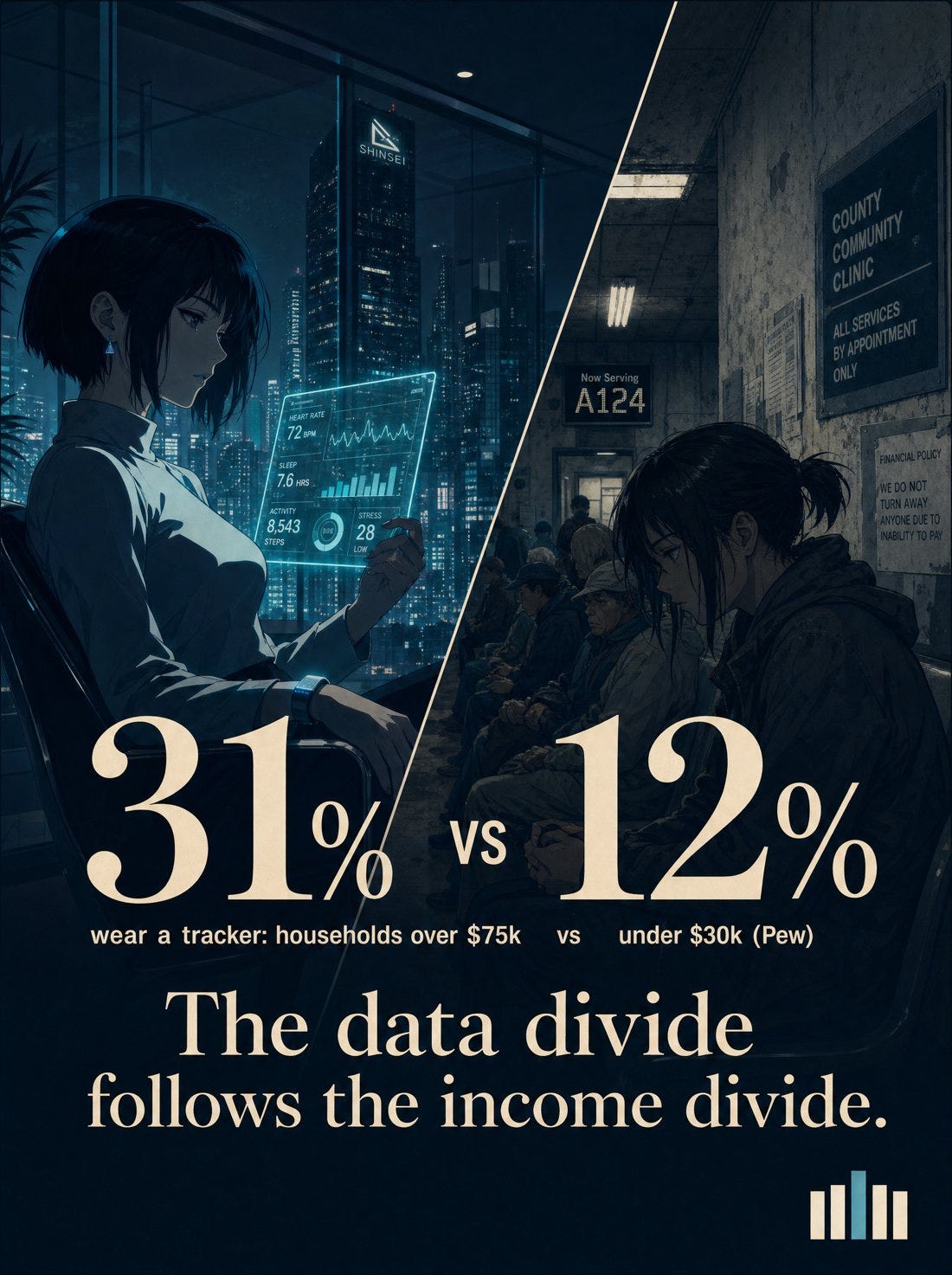

The price of entry, and the gap it produces. A leading wearable runs $199 to $359 a year; tracker use runs 31% in households over $75k against 12% under $30k.8
ii.The data is biased, and the model will be too
A distribution problem becomes a clinical-AI problem here. The longitudinal data now training risk models comes disproportionately from the connected and the comfortable. In the ABCD study, Black children were markedly underrepresented among those who shared wearable data and wore the devices for fewer days, and low-income households were underrepresented too. The datasets teaching machines what “normal” physiology looks like carry that skew from the start.9 The Lancet Digital Health put the warning on the record. The Apple Heart Study, for all its scale, required owning an Apple product, which biased it toward a “young, wealthy, and technology-proficient” population, and algorithms built on such cohorts generalize poorly to everyone else.10
If clinical AI learns from the people who need it least, it will work best for the people who need it least.
iii.The broadband floor
Solve cost tomorrow and put a device on every wrist, and the signal still has to leave the home. About 28% of rural Americans lack access to high-speed broadband, and counties with lower broadband and higher social vulnerability show measurably lower telemedicine use, with Medicaid recipients consistently less likely to connect.11 Put that on a rural map where the hospital itself is disappearing, with 182 rural hospitals closed or stripped of inpatient care since 2010,12 and the failure mode turns concrete. When the hospital closes and the broadband never arrived, the algorithm does not drive out to meet the patient. It never sees them.

iv.The ACCESS Model: a real lever, and a subtle selection problem
A new federal model is directly relevant to this, and goes live this week. The CMS Innovation Center’s ACCESS Model, short for Advancing Chronic Care with Effective, Scalable Solutions, is a voluntary ten-year experiment in Medicare fee-for-service that begins in July 2026. It pays for technology-supported chronic care: remote monitoring, connected devices, and the staff time around them.13
I discussed in detail how the model only functions with deep integration of tech enabled care, alignment with referring entities, and AI native deployments. RevelAi health is launching our MSK ACCESS Care Model this week, and we are slated to engage thousands of patients in the first few months of the program along referring entities we have partnered with. The model has could veritably expand the front door to chronic care, but there are pitfalls to anticipate as well.
AI Care or Bust: The CMS ACCESS Model Operator's Playbook

For those catching up, I wrote a 12-part Techy Surgeon operator series on the CMS ACCESS Model. To navigate this series start to finish, check the archives if you’re a subscriber or check out this page on Techy Policy.
ACCESS replaces ordinary fee-for-service billing for a qualifying condition with what CMS calls Outcome-Aligned Payments. A participating organization takes a predictable, risk-adjusted payment to manage a condition such as hypertension or type-2 diabetes, and collects the full amount only when patients reach a measurable target, a lower blood pressure or a reduced pain score. To keep that workable, CMS scores performance on the share of an organization’s panel that hits target, so a group can still earn full payment on strong overall results even if some individual patients fall short. CMS will publish each participant’s risk-adjusted outcomes and run a public directory, so patients and primary-care physicians can pick a participant by performance and condition.14 A rural adjustment raises reimbursement for rural patients and providers, a deliberate pull toward the places that usually get skipped.13
The rural adjustment is an excellent instinct from the administration on this model. Though the scoring rule has a slippery side effect that isn’t accounted for today. When payment depends on the share of patients who reach target, the safest way to lift that share is to enroll patients likely to engage and succeed: the ones with broadband, a charged device, and time to answer a nudge. “Appropriate patients” can slide toward “patients who will make our numbers.” Value-based care has carried this cream-skimming risk for two decades, and a technology whose adoption already follows income sharpens one end of the double-edge sword of accountable care.
The tension in one line
ACCESS pays for outcomes and for the share of patients who reach them. Wearable engagement already skews wealthy, connected, and well. Without a strong correction, the cheapest way to make the numbers is to enroll the patients who were going to do fine anyway, which inverts the model’s intent.
v.The experiment should expand
My thoughts as we prepare to deploy. This model has tremendous paradigm shifting potential. The advent of clinical AI is shifting the front door upstream. Keep the outcome-based payment; it can work. The task is to make caring for the hardest patients the profitable choice. Three moves get there.
Extend it to Medicaid. The continuous-data work is being piloted almost entirely in Medicare and the commercial market, while the population with the steepest chronic-disease burden and the thinnest access sits mostly outside the experiment. The rural-bonus instinct, applied to Medicaid and to complex dual-eligible patients, would put the tool where the need runs highest.
Add a Maintenance for Mobility, Fall Prevention, and Bone Health in the MSK Track. This is a moderate to severe miss on the model. The MSK track does not have a maintenance track. Medicare patients with musculoskeletal conditions that are well documented to recur are on a constant churn, and there is a missed opportunity to hone in on durable care gap closure of bone health and fall prevention that could save Medicare millions.
On JAMA's ACCESS Perspective: Bone Health Was the Missed Track

Jacob Shiff and Abe Sutton at the CMS Innovation Center published a JAMA Perspective today walking through the logic behind the ACCESS Model and Outcome-Aligned Payments [1]. It is a fairly clear articulation of how the team thought about this model and worth a read.
Risk-adjust for reality. An organization that takes on a low-income rural patient with five conditions, social drivers of health, and no broadband should be paid for the attempt and the trajectory, not only the finish line, and the payment should cover what closes the gap: the device, the connectivity, and the human coaching the evidence keeps pointing to.4 Risk adjustment that ignores social complexity does more than underpay. It signals which patients to avoid.
Believe the proof. Remote monitoring with CGM at a safety-net hospital in the Bronx produced a 3.0-point HbA1c drop against 2.1 in usual care, more than doubling the odds of reaching goal.15 A connected-device, health-coaching program at a rural California community health center, two-thirds Spanish-speaking, cut systolic blood pressure by 20 mmHg.16 The EXTEND trial enrolled persistently uncontrolled, mostly Black patients and built on the infrastructure clinics already had, so it could scale to the people usually left out.17 The underserved benefit when someone builds the access and the wraparound for them. Almost no one has. We will at RevelAi Health. Empower more organizations to be incentivized to do the same.

vi.The test for the insurgents
That leaves the companies racing onto this surface, facing two roads. The first is easy and lucrative: sell continuous optimization to the worried well, collect a subscription, raise on a graph going up and to the right, and call a widening gap growth. The second is slower: build for the disconnected and the complex, where the unmet need runs largest and where a model paid on real improvement has the most room to move a number that matters. I personally choose the latter, and I hope the health tech operators who read this newsletter will do the same.
Wearables, longitudinal data, and outcome-aligned payment could finally bend chronic disease in the populations the system has failed for decades. Or they become one more frictionless luxury delivered to the people who least need it. CMS can tilt the incentive, and the rural bonus shows it knows that. The builders still have to choose the harder road on purpose.
Sources
Every empirical claim above links to a primary source. Peer-reviewed evidence via PubMed / Consensus; policy detail from CMS; population figures from federal data.
Martens T, et al. Effect of CGM on glycemic control in T2D treated with basal insulin: a randomized clinical trial. JAMA (2021).
Uhl S, et al. Effectiveness of CGM on glycemic control in T2D: systematic review & meta-analysis of RCTs. J Clin Endocrinol Metab (2023).
Kelly F, et al. Effect of telehealth on clinical outcomes in hypertension and diabetes: a meta-analysis of 106,261 patients. J Telemed Telecare (2024).
Noah B, et al. Impact of remote patient monitoring on clinical outcomes: an updated meta-analysis of RCTs. npj Digital Medicine (2018).
Nagappan A, et al. Patterns of ownership and usage of wearable devices in the United States, 2020–2022. J Med Internet Res (2024). (Income ≥$200k OR 2.27; Medicaid 0.75×; uninsured 0.41×; rural 0.65×.)
Chandrasekaran R, et al. Patterns of use and key predictors for the use of wearable health-care devices by US adults. J Med Internet Res (2020).
Stewart L, et al. Current patterns of use and acceptability of consumer wearable activity trackers in ED patients. J Exerc Nutr (2024).
Pew Research Center. Smartwatch / fitness-tracker use by income (31% of $75k+ vs 12% of under $30k). Membership pricing: WHOOP ($199 / $239 / $359 per year); U.S. Census, median household income $83,730 (2024).
Kim E, et al. Association of demographic and socioeconomic indicators with the use of wearable devices among children. JAMA Network Open (2023).
Zinzuwadia A, Singh JP. Wearable devices and addressing bias and inequity. Lancet Digital Health (2022).
Social vulnerability, lower broadband internet access, and rurality associated with lower telemedicine use in U.S. counties (PMC, 2025); FCC broadband-access estimates (≈28% of rural lacks high-speed broadband).
Chartis. 2025 Rural Health State of the State (182 rural hospitals closed or dropped inpatient care since 2010).
CMS Innovation Center. ACCESS (Advancing Chronic Care with Effective, Scalable Solutions) Model (voluntary 10-year Medicare FFS model beginning July 2026; rural adjustment for patients and providers).
CMS. Improving ACCESS to technology-supported care with Outcome-Aligned Payments (full payment when patients meet outcome goals; scored on share of patients meeting targets; public directory of risk-adjusted outcomes).
Cuan K, et al. RPM with CGM improves glycemic outcomes in T2D at a safety-net hospital. Endocr Pract (2025). (HbA1c −3.0% vs −2.1%; goal OR 2.53.)
Kim KK, et al. Improving hypertension and diabetes outcomes with digital care coordination and remote monitoring in rural health. (2025). (Rural CHC; SBP −20 mmHg.)
German JC, et al. EXTEND: technology-enabled, nurse-delivered chronic-disease care, protocol and baseline data for an RCT. Contemp Clin Trials (2024).
Interesting article from a UK perspective. The model is very different, obviously, from your system, versus our centralised health service. But the problem you're naming shows up here too, just earlier in the chain.
We already have the trackers. Lots of different devices, lots of different standards, all collecting data that nobody downstream can do anything with. Turn up at a GP with your own numbers and the honest answer is: what am I supposed to do with that? There's no mechanism for consuming it, and no trust in it either — there's still no verifiable source for what any of these devices actually capture.
Go to A&E and the gap gets sharper. Clinicians don't have time to review a wearable history. They want evidence taken while you're in front of them, not a heart-rate reading from a device with no idea what you were doing when it recorded it. That's a long way from anything that could trigger a medical emergency directly. If someone is having an anaphylaxis event, how does that reach a 999 service — where, when, why, and how?
There's a sharper risk sitting underneath all of this: a two-tier health service that goes further than the bias we already have. Have a device, and you can hand a clinician usable evidence. Don't have one, and you're assessed on less information than the person next to you — treated worse for having less to offer, not for being less unwell.
That's not a niche question. It sits directly on the UK's digital divide. A wearable isn't a purchase most families can weigh against heating the house or feeding the kids — it's not a choice available to them at all. Any universal system that starts rewarding the data-rich needs an honest answer for what happens to the person who was never able to buy their way into being visible.
Your wearable-ownership gap is one design failure. The absence of any agreed way for a GP or paramedic to actually use the data once it exists is another, sitting immediately downstream of it — and nobody seems to own that one either.